Each week in the lead up to Accreditation, Northern Health will focus on a different Standard. You will hear from the Chairs of each Standard Committee on what you need to know.
This week we spoke to Lora Davies, Divisional Director, Sub-Acute Services & Access, about Standard 6: Communicating for Safety.
What is this standard about?
Standard 6 is all about Communicating for Safety. The three main areas this covers are:
- Patient Identification
- Procedure Matching
- Clinical handover
But, as you can imagine, the need for clear and timely communication is required in almost every part of our organisation. We aim to ensure that the patient is provided with timely, purpose-driven and effective communication and documentation that support continuous, coordinated and safe care for patients.
At Northern Health, this standard looks like….
Some examples:
- Checking patients 3 points of identification
- Ensuring appropriate safety checklists are completed prior to procedure matching (surgery, endoscopy, ophthalmology, etc)
- Bedside nurse handover at end of shift
- ISBAR Handover between clinicians at points of transfer of care (ward to ward, etc)
- Identifying and acting upon new critical information about your patient
What are the top 5 ways staff can be prepared for Accreditation against this Standard?
- Have a think about what the term ‘critical information’ means for your area.
- Ensure your patients have access to bedside patient communication boards.
- Ensure you are involving patients and carers in decision making – via effective communication.
- Ensure your team are handing over the right information for each patient.
- Ensure handover sheets aren’t left in public areas.
What are the top 5 questions staff needs to be able to answer about this Standard?
- How do you define critical information in your area?
- How do you ensure patients are able to engage in their care and decision making?
- What processes do you use to ensure you are identifying the patient correctly?
- What processes do you use to ensure you are performing the right procedure on the right patient?
- Are you ensuring your handovers are done in ISBAR format?
Is there anything else you would like staff to know about this Standard?
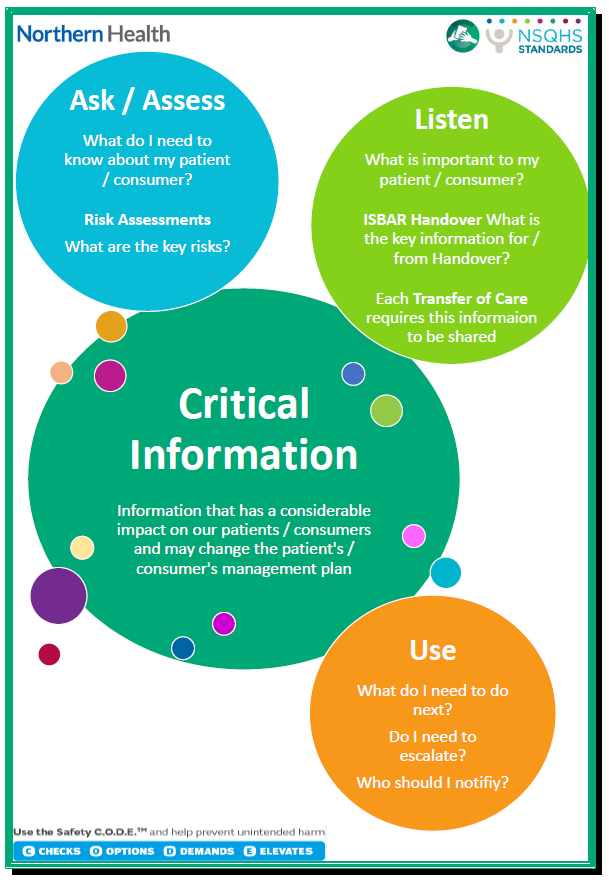
Standard 6 has been focusing on supporting clinicians in defining ‘critical information’.
Critical information can be something that is known (i.e. alerts/allergies), it could be something that is new information (i.e. patient mentions it at some point in their care), or it could be something that we actively seek out such as identifying risks within iView of EMR or the relevant paper based documents, or asking specific questions.
When new critical information arises, it should be addressed as soon as possible via appropriate clinical action. We also acknowledge that critical information looks different in each setting. The below Fact Sheet has been developed to assist.